
Canine heart disease is estimated to occur among 10 % of all dogs in primary practice (Atkins et al. 2009). Heart disease is especially prevalent in small breed dogs (Borgeralli et al. 2008, Mattin et al. 2015) with chronic degenerative valve disease (CVD) being by far the most common type of acquired heart disease (Baumgarten & Glaus 2004, Elsharkawy et al. 2022).
Most patients with chronic degenerative valve disease are clinically asymptomatic and continue to be for a long time (Borgarelli et al. 2008), with only about 30 % of them progressing into heart failure and death because of heart disease (Borgarelli & Haggstrom 2010). For those canine patients that progress into congestive heart failure, an important at-home monitoring includes the resting respiratory rate (RRR). Stabile patients most often have a RRR below 30 breaths per minute (Porciello et al. 2016). In the clinical setting a respiration rate below 40 breaths per minute would indicate stability (Schober et al. 2010). Through published guidelines from the American College of Veterinary Internal Medicine (ACVIM), patients with CVD can be staged and recommendations regarding therapy are advised (Keene et al. 2019).
History
A nine-year-old entire male Chihuahua presented to the clinic with acute onset of increased respiratory sounds, and for the last couple of days also an aggressive behavior towards the owner. The dog’s appetite and water intake were normal, but it had regurgitated some white foam. There was no previous history of illness or medication. The dog was up to date on its vaccinations.
Clinical Findings
On clinical examination the dog seemed anxious and was in respiratory distress with a restrictive respiratory pattern. It had rapid and shallow breathing and was tachypneic with a respiratory rate of 104 breaths per minute. Mucous membranes were mildly cyanotic, capillary refill time was less than 2 seconds. Dental status was bad. Body condition score was normal with a body weight of 3.1 kg. On auscultation a grade 4 out of 6 systolic murmur was heard, loudest on the left side of the thorax at the apex. The heart rate was normal, 112 beats per minute. Increased lung sounds and crackles were heard on both sides of the thorax. Femoral pulses were of normal strength. Body temperature was normal, 38.5 °C. There were no other clinical findings.
Problem list and differential diagnoses
The clinical examination revealed the following problem list:
- Dyspnea and tachypnoea characterized by a restrictive respiratory pattern, increased lung sounds and crackles
- Mildly cyanotic mucous membranes
- Grade 4 out of 6 systolic murmur, maximum intensity at the left apex
- Regurgitation of foam
- Dental calculus and gingivitis.
Differential diagnosis respiratory signs:
- Pulmonary edema from congestive heart failure
- Pneumonia
- Pulmonary fibrosis
- Pleural effusion from pleural space disorders
- Pneumothorax
- Neoplasia.
Differential diagnoses heart murmur:
- CVD
- Congenital heart disease, i.e. mitral valve dysplasia
- Mitral valve endocarditis
- Dilated cardiomyopathy
- Myocarditis.
Differential diagnosis regurgitation of foam:
- Gastroesophageal reflux
- Esophagitis
- Megaesophagus
- Foreign body
- Dysphagia
- Endocrine disorders.
Differential diagnosis dental findings:
- Periodontitis
- Endodontic disease.
Dental disease was not addressed further as it was assessed not to influence the outcome and short-term prognosis for the patient.
Diagnostic Techniques
The acute respiratory distress of the patient was assessed to be a clinical emergency and shortly after presentation an intravenous catheter was placed to give both 0.03 mg/kg butorphanol (Butomidor 10mg/mL solution for injection; Salfarm Denmark) intravenously (iv) and 2 mg/kg furosemide (Furix 10 mg/mL solution for injection; Accord) iv. The butorphanol calmed the dog enough to tolerate an oxygen mask and to allow blood sampling with minimal stress. Thoracic radiographs were taken with digital X-ray (Visaris Avanse Vision Vet) as a dorsoventral view and left and right lateral views. The dog was still tachypneic and therefore handled with minimal stress. On laterolateral views an enlarged cardiac silhouette was present, pushing the trachea dorsally (figure 1 and 2).
Tenting of the left atrium was seen together with dilation of the pulmonary veins cranial to the cardiac silhouette (figure 2). A diffuse alveo-interstitial lung pattern was present, most pronounced at the hilus region and in the caudodorsal lung field, suspicious of cardiogenic pulmonary edema. In the left laterolateral view an interlobar fissure line was visible in the caudal lung field (figure 2). The dorsoventral view confirmed the presence of interlobar fissure lines indicative of some degree of pleural effusion (figure 3). Cowboy leg-appearance of the main stem bronchi was seen, indicating enlargement of the left atrium. From the right laterolateral radiograph the vertebral heart score, VHS, and vertebral left atrial size, VLAS, were measured as 10.7 and 3.2, respectively (reference range VHS<10.5 and VLAS<3, Keene et al. 2019). Aerophagia was seen with a gas-filled ventricle.
(The article continues after the pictures).

Figure 1. Right laterolateral radiograph showing enlarged cardiac silhouette, dorsal displacement of the trachea (orange arrow), tenting of the left atrium (green arrow) and an alveo-interstitial lung pattern.

Figure 2. Left laterolateral radiograph with same findings as figure 1 and furthermore showing more visible dilation of the pulmonary veins cranial to the cardiac silhouette (blue arrow) and an interlobar fissure line in the caudal lung field (yellow arrow). The ventricle is gas-filled (black arrow).

Figure 3. Dorsoventral radiograph showing the cowboy leg-appearance of the main stem bronchi (white arrows) and interlobar fissure lines (yellow arrow).
Hematology results came back with a mild leucocytosis 19.13x10^9/L (reference range 5.05-16.76) characterized by mild neutrophilia 15.18x10^9/L (reference range 2.95-11.64) and mild monocytosis 1.34x10^9/L (reference range 0.16-1.12). Furthermore, a mild reticulocytosis 141.6 K/µL (reference range 10-110) was seen.
Serum biochemistry showed a creatinine result below normal, 39 µmol/L (reference range 44-159) and a mild elevation in ALT, 218U/L (reference range 10-125) and GGT, 19U/L (reference range 0-11). Serum electrolytes showed moderate hyperkalemia 6.2mmol/L (reference range 3.5-5.8). Blood results are shown in figure 4.

Figure 4. Blood results.
Diagnosis
The patient presented with acute dyspnea and tachypnea with a grade 4 out of 6 systolic heart murmur. Thoracic radiographs showed the three hallmarks of congestive heart failure:
- Enlarged left atrium
- Dilated pulmonary veins
- Loss of detail as a result of an alveo-interstitial lung pattern.
There were also signs of mild pleural effusion.
Hematology and biochemistry showed changes that can be seen in patients with congestive heart failure without signs of further complications. Blood results are reflected upon later.
The patient was diagnosed with acute congestive heart failure. A characterization of the underlying heart condition was not possible until the patient had been stabilized. Echocardiography was performed 6 days later.
The regurgitation noted was suspected to be explained by aerophagia due to respiratory distress. Signs of regurgitation were not seen again once the patient was stabilized.
Case Management
The initial treatment of the patient focused on stabilization of its congestive heart failure. Mild sedation with a single dose 0.3mg/kg butorphanol iv and repeated intravenous furosemide at a dosage of 2mg/kg was instituted together with flow-by oxygen until respiratory rate and respiratory effort normalized (table 1). Concurrently, both mucous membrane color and the overall well-being of the dog improved.
|
Time in hours |
Respiratory rate, RR |
Treatment |
|
0 |
RR 104/min |
2 mg/kg furosemide iv, 0.03 mg/kg butorphanol iv |
|
1 |
RR 104/min |
2 mg/kg furosemide iv |
|
2 |
RR 67/min |
2 mg/kg furosemide iv |
|
3 |
RR 54/min |
2 mg/kg furosemide iv |
|
4 |
RR 36/min |
None, improvement seen, increasingly difficult to handle the patient |
|
5 |
RR 40/min |
2 mg/kg furosemide iv |
|
6 |
RR 40/min |
0.32 mg/kg torasemide po and 0.2 mg/kg pimobendan po |
Table 1. Acute treatment schedule, iv: intravenous, po: peroral.
Simultaneously with improvement in respiratory rate, the dog gained back its normal behavior towards strangers, which was growling and difficulty with handling. The respiratory rate did not improve from 36-40 breaths per minute despite repeated intravenous furosemide dosage and an improvement in breathing pattern. To minimize stress, the dog was switched to oral treatment, sent home for the night and scheduled for check-up next morning. The oral treatment given was high dosage torasemid 0.32 mg/kg (Isemid 1 mg tablets; Ceva Animal Health A/S) and pimobendan 0.2 mg/kg (Vetmedin 1.25 mg tablets; Boehringer Ingelheim Animal Health Nordics A/S).
Improvement continued at home during the night. The owner reported that the dog showed normal behavior. On clinical examination the following morning the dog was difficult to handle. The respiratory rate was 40 breaths per minute. Thorough clinical assessment of the patient was difficult. Thoracic radiographs were repeated for more information. The alveo-interstital lung pattern had improved and the interlobar fissure lines were almost not visible anymore (figure 5-7). This indicated that the pulmonary edema and pleural effusion were resolving. The ventricle was also markedly less gas-filled.
(The article continues after the pictures).
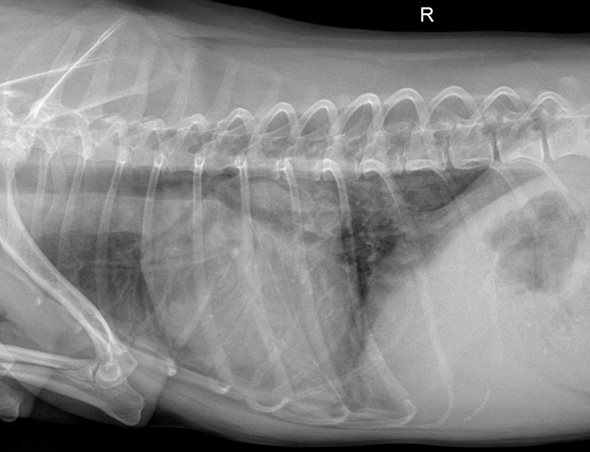
Figure 5. Right laterolateral view 24 hours from first furosemide dosage, showing improvement of the alveo-interstitial lung pattern. This indicates resolvement of the pulmonary edema.
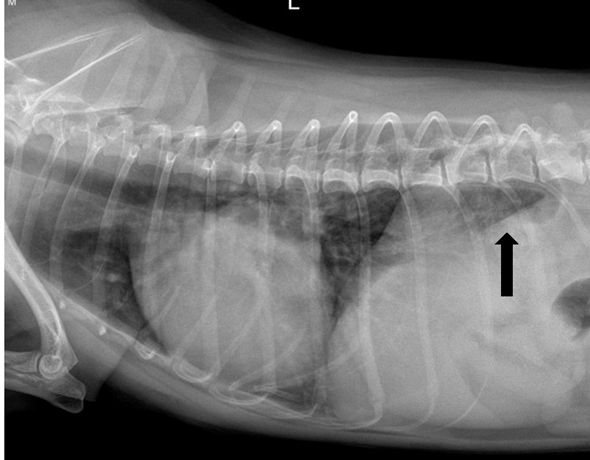
Figure 6. Left laterolateral view 24 hours from first furosemide dosage showing improvement of the alveo-interstitial lung pattern. This indicates resolvement of the pulmonary edema. Note the markedly less gas-filled ventricle (black arrow).
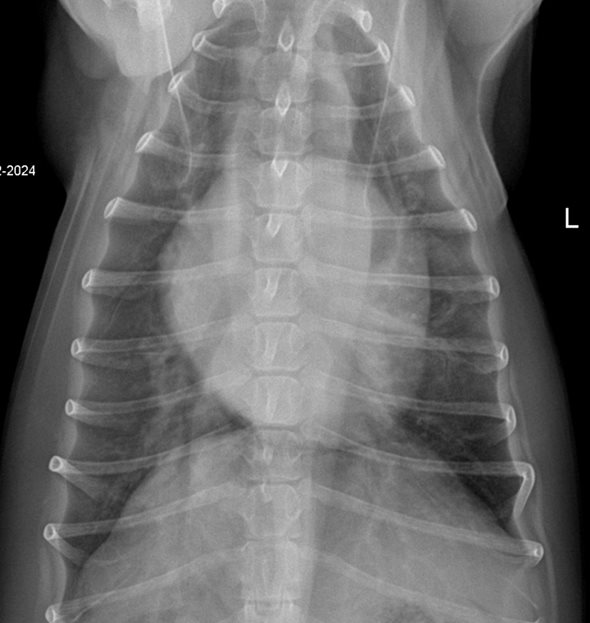
Figure 7. Dorsoventral view showing improvement of the alveo-interstital lung pattern and of the interlobar fissure lines. This indicates resolvement of the pulmonary edema and pleural effusion.
Torasemide at 0.32 mg/kg orally once daily was continued for 5 days total and then reduced to 0.16 mg/kg once daily. Pimobendan was continued at 0.2 mg/kg twice daily orally.
Echocardiography was performed 6 days from the acute presentation (MylabEasoteX8, phased array probe 2-9 MHz). Right parasternal long and short axis view, subcostal view and left apical four and five chamber views were used. A mitral regurgitation was found with thickening of the valvular leaflets, especially the anterior mitral valve leaflet (figure 12). There was significant dilation of the left ventricle and left atrium (figure 9-10), with a normalized left ventricular internal diameter in diastole (LVIDDn) of 1.9 and a left atrium to aorta ratio (LA/Ao) of 2.0 (reference LVIDDn <1.7 and LA/Ao <1.6, Keene et al. 2019).
(The article continues after the pictures).

Figure 8. Measurements performed on echocardiography.

Figure 9. Right parasternal short axis view at the level of the aortic valve showing the measurement of the ratio of left atrium (LA) to aorta (Ao).

Figure 10. Right parasternal short axis view at the level of the papillary muscles, M mode, measuring left ventricular dimensions, LV: Left ventricle.
Systolic function was high-normal for a Chihuahua, with an ejection fraction (EF) of 89 % and a fractional shortening (FS) of 58 % (Niimi et al. 2022). Diastolic function was decreased showing restrictive filling. The E velocity was high, 1.5m/s (figure 11), and the ratio of E to isovolumetric relaxation time (E/IVRT) was 4.2 (figure 8). B lines were visible just across the heart base bilaterally but not anywhere else.

Figure 11. Left apical four chamber view measuring diastolic filling with pulsed wave Doppler. LA: Left atrium, LV: Left ventricle, RA: Right atrium, RV: Right ventricle. The E velocity is the tall wave marked by a blue arrow.

Figure 12. Left apical four chamber view with left side of the heart in focus, showing thickening of the mitral valves, especially the anterior mitral valve, which has a club shaped appearance.
An electrocardiogram (ECG) was performed simultaneously and showed a regular sinus rhythm throughout the echocardiography.
The underlying heart disease was diagnosed as CVD with restrictive filling pattern. As the patient presented to the clinic in acute congestive heart failure, the classification of the CVD according to ACVIM was stage C.
Ideally a follow-up blood sample should have been part of the protocol to assess electrolytes and renal values on torasemid treatment, but the owner rejected further stressful events as the dog was now stabile and doing well. Instead, daily monitoring of RRR at home was instituted as well as monthly clinical assessment. The patient’s therapy was supplemented with oral spironolactone 2.9mg/kg and benazepril 0.37mg/kg once daily (Cardalis 2.5 mg/20mg tablets; Ceva Animal Health A/S). The diet was switched to a veterinary cardiac diet. Owner was informed of a guarded prognosis with risk of repeated relapse of congestive heart failure and a mean survival time of approximately one year (Brložnik et al. 2023, de Madron et al. 2011, Häggström et al. 2008).
Progress and outcome
During the next 3 months the patient was stabile. The respiratory rate was 24 breaths per minute at home and 40 breaths per minute at the veterinary clinic. At one point the owner complained about relapse of aggressive behavior at home and a small increase in RRR to 28 breaths per minute. The dog had gained some weight, now weighing 3.4 kg, making torasemide dosage with half a tablet relatively low. Torasemide dosage was increased to 0.29 mg/kg (1 tablet). The heart condition was stabile for another 3 months, then suddenly another increase in RRR was observed at home. Clinically respiratory rate had also increased, 48 breaths per minute, and heart rate was increased to 120 beats per minute. Normal lung sounds were heard on auscultation. Blood pressure measurement was performed before any further adjustments in therapy.
Five measurements were made. The mean of the three middle measurements was calculated to be 125 mmHg systolic pressure. The patient was concluded to be normotensive and therefore diuretic therapy was increased. Torasemide was increased to 0.44 mg/kg once daily for 5 days and then switched down to 0.29 mg/kg once daily again. The following two months the dog had 4 episodes of increases in RRR which were controlled in the same way. The dog had progressed to ACVIM stage D refractory heart failure and euthanasia was elected 8 months from the acute presentation.
Discussion
Acute dyspnea and tachypnea in a small breed dog with a loud, untreated heart murmur is indicative of acute congestive heart failure (Herrtage 2010, Ware 2003). The gender and age of the patient correlates with previously reported data showing increased prevalence of CVD in small breed male senior dogs (Borgeralli et al. 2008, Mattin et al. 2015). Differential diagnoses included lung parenchymal diseases and pleural space disorders. The findings on the thoracic radiographs led to increased suspicion of cardiogenic pulmonary edema with increased VHS and VLAS indicating significant enlargement of the left side of the heart (Keene et al. 2019). Response to diuretic treatment confirmed suspicion of the diagnosis and echocardiography provided a diagnosis of the underlying heart disease.
Studies have shown that some measures of diastolic filling pressure can be used as prognostic markers for an increased risk of developing congestive heart failure from chronic degenerative valve disease. These measures are E/IVRT >2.5 and Evel>1.2 m/s, respectively (Borgarelli et al. 2008, Schobert et al. 2010). In the present case the patient had values above the cut off levels from these studies (figure 8) and was indeed in acute congestive heart failure.
The patient’s hematology showed mild neutrophilia and mild monocytosis, which are findings of a stress leucogram. Reticulocytosis is seen in dogs with cardiogenic pulmonary edema due to hypoxia (Choi et al. 2022).
Biochemistry showed a mild elevation in ALT. Mild elevations in liver enzymes are seen in congestive heart failure due to hypoperfusion and hypoxia of the tissue (Patowary et al., 2022).
Usually, azotemia is seen with congestive heart failure (Nicolle et al., 2007, Patowary et al., 2022). Creatinine level can increase further with the use of loop diuretics (Besche et al. 2020, Giorgi et al. 2022, Nicolle et al. 2007). The patient in the present case had a low creatinine level, which could be explained by age and size. Misbach et al. (2014) showed that creatinine levels trend lower in small-sized dogs, and Hall et al. (2017) have shown a reduction in creatinine levels with reduced lean body mass as occurs with increased age. Torasemide was chosen as the oral diuretic for increased compliance as it only had to be administered once daily, and the lowest effective dosage was used for long term treatment. Torasemide has been shown to be noninferior to furosemide (Besche et al. 2020). The patient had hyperkalemia at the time of the acute congestive heart failure.
More often patients in congestive heart failure are normokalemic (Patowary et al. 2022, Roche-Catholy et al. 2021). It is important to monitor electrolyte status when initiating therapy, as treatment with furosemide tends to lower potassium levels of the patients (Brložnik et al. 2023). The patient in the present case was stressed with handling. Repeated blood sampling would indeed be very stressful. Therefore, it was decided that close at-home and clinical monitoring would be appropriate as first line assessment. Furthermore, the potassium-sparing diuretic spironolactone was initiated 6 days after furosemide as part of the treatment protocol recommended for CVD ACVIM stage C (Keene et al. 2019). But the best practice approach would have been to measure renal values and electrolytes ongoing.
Thoracic radiographs showed a small amount of pleural effusion, which usually indicates some degree of right sided congestion as well as the obvious left sided congestive heart failure that was present. Echocardiography showed no signs of tricuspid regurgitation or right sided enlargement, i.e., no pulmonary hypertension was found. According to Beatty and Barrs (2010), the visceral pleura drains into the pulmonary veins in both cats and dogs making possible some degree of pleural effusion from increased congestion of the pulmonary veins present in left sided congestive heart failure. This is much more commonly seen in cats, though.
As expected from the findings in the study from Porciello et al. (2016), monitoring of the RRR at home was fundamental in the follow-up period for the patient in the present case. It proved to be a simple, but very efficient tool for adjusting therapy to improve quality of life and survival time in a patient that was very stressed in the clinical setting.


